
Groin hernia repair is associated with excellent short- and long-term outcomes, but complications of the procedure exist and must be recognized. The most important are Recurrence, Infection and Neuralgia, though injuries to the bladder, testicle or vas deferens can also occur.
Recurrence
Recurrence of the hernia in the early postoperative setting is rare. When this does occur, it is often secondary to deep infection, undue tension on the repair, or tissue ischemia. Clearly, all of these etiologies raise the concern for a technical complication on the part of the surgeon, either in the handling of the groin tissues or the placement of mesh or suture. The patient who is overactive in the immediate postoperative setting may also be at risk for early hernia recurrence. In this way, it is thought that early exercise is performed before the suture or mesh in the repair has had an opportunity to hold tissue in place and promote scar tissue formation. In the initial postoperative setting, patients may also develop seromas along the planes of dissection as well as fluid in the obliterated hernia sac. These benign consequences of surgery must be differentiated from the more worrisome early recurrence.
Tension is an important, if not the primary, etiology of hernia recurrence. Tissues repaired under undue tension will tend to pull apart, even if sutures or mesh have been affixed to them. In addition, tension at the site of suture may lead to ischemia at the point where the suture pulls against the tissue, thereby further weakening the hernia repair. Sutures can also cut out or fall apart, especially if placed in a continuous fashion, when tensile force predominates. The role of excessive tissue tension in promotion of hernia recurrence is the basic rationale behind the modern, tension-free and increasingly suture-free hernia repairs advocated by hernia experts such as Lichtenstein and Rutkow.
Infection
Infection of the hernia wound or mesh is an uncommon postoperative complication but represents another etiology of hernia recurrence. In specialized hernia practices, the incidence of wound infection following inguinal hernia operation is 1% or less. When an infection does occur, skin flora are the most likely etiology, and appropriate gram-positive antibiotics should be initiated. Patients who undergo mesh placement during groin herniorraphy are at a slightly higher risk of postoperative wound infection. It is often difficult to determine whether the mesh itself is infected or if just the skin or soft tissue anterior to the layer of mesh is infected. However, even if mesh is present, most postoperative groin hernia infections can be treated with aggressive use of antibiotics after the incision is opened and drained expeditiously. Mesh removal in this setting is rarely indicated; when this is mandated, primary closure or redo herniorraphy with a synthetic tissue substitute may be warranted and a preperitoneal approach may be necessary.
Neuralgia
Postoperative groin pain, or neuralgia, is common to varying degrees following groin herniorrhaphy. Often, the neuralgia will follow the known distribution of the regional nerves, including the ilioinguinal, iliohypogastric, genital branch of the genitofemoral nerve, and the lateral femorocutaneous nerves. During open hernia repair, the ilioinguinal, iliohypogastric, and the genitofemoral nerves are most commonly injured, while the lateral femorocutaneous nerve is more commonly injured during laparoscopic herniorraphy. Nerve injury is usually due to entrapment of a portion of the nerve in the mesh or suture line placed in one of the soft tissue layers.
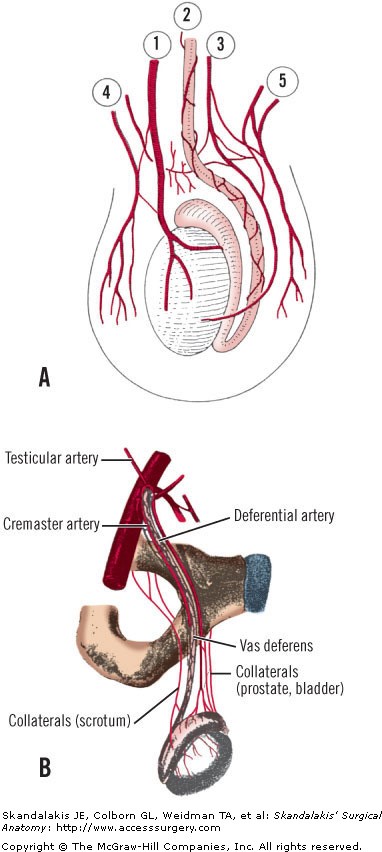
Figure Legend: Complications of the testis can occur from damage to the relevant arterial supply, the arteries of the testis and epididymis. A, The testicular artery (1) is the chief source of blood to the testis, but four other arteries anastomose with the testicular artery and each other to form a collateral circulation. 2, Deferential artery; 3, Cremasteric artery; 4, Posterior scrotal artery; 5, Anterior scrotal artery. B, The principal blood supply of the testicle is from the testicular artery, which arises from the aorta or the renal artery. The testicle also receives blood from the artery of the vas deferens, which arises from the internal iliac artery, and from the cremasteric artery, which originates from the external iliac artery. The cremasteric artery supplies blood to the cremaster muscle and to the tunica of the testicle. A rich collateral circulation exists between the testicle and the arteries to adjacent structures, such as the prostate, scrotum, etc. (A, Modified from Skandalakis JE, Gray SW, Rowe JS Jr. Anatomical Complications in General Surgery. New York: McGraw-Hill, 1983; with permission. B, Courtesy of GE Wantz [modified].)
Board Review Questions
1. The least common reason for recurrence of a groin hernia within the first year after repair is
A. Overlooking an indirect hernia sac
B. Tension on the fascial repair
C. A missed femoral hernia
D. Failure to close the fascial defect adequately
E. A defect in collagen synthesis
2. Factors associated with a laparoscopic inguinal hernia repair compared to an open repair include all of the following except
A. Less postoperative pain
B. Faster return to work
C. Longer operative time
D. Requires general anesthesia
E. Lower cost
3. Of the following, the groin hernia that is most likely to incarcerate and strangulate is a
A. Femoral hernia
B. Indirect inguinal hernia
C. Direct inguinal hernia
D. Pantaloon hernia
E. Amyand hernia
Answers
1. The correct answer is E. A defect in collagen synthesis
2. The correct answer is E. Lower cost
3. The correct answer is A. Femoral hernia

Create a Free MyAccess Profile
AccessMedicine Network is the place to keep up on new releases for the Access products, get short form didactic content, read up on practice impacting highlights, and watch video featuring authors of your favorite books in medicine. Create a MyAccess profile and follow our contributors to stay informed via email updates.