
Historically, administering general anesthesia without endotracheal intubation was uncommon. While this approach avoids the complications of intubation, it has many disadvantages. If the patient vomits even a small amount, the airway is unprotected and aspiration will occur. Furthermore, the anesthesiologist must hold the mask with one hand during the entire procedure, and this hinders performance of the many other tasks required (e.g., administration of other drugs or blood, record keeping, and monitoring). With the use of the laryngeal mask airway (LMA) (see below), administration of anesthesia via a mask is increasingly rare.
Approach to Airway Management Other Than Traditional Endotracheal Intubation
In the last 10 years, many other options have become available for managing the airway in both the awake and the anesthetized patient. The two most important are the LMA and the fiberoptic laryngoscope. The LMA is an alternative to endotracheal intubation when less invasive approaches are desired or when endotracheal intubation is difficult or impossible; it provides an excellent airway but does not protect against pulmonary aspiration of gastric contents. The fiberoptic laryngoscope represents a major advance in the management of difficult airways in both awake and anesthetized patients. Other valuable but less often used devices include the lighted stylet (lightwand) and the Bullard intubatory laryngoscope as well as many types of endotracheal tests. Since the introduction of the LMA, many derivatives have been developed, including the intubating LMA, the Pro Seal LMA, the Combitube, and many others—all designed to overcome disadvantages of the original LMA or extend its clinical opportunities.
Indications for Endotracheal Intubation
Endotracheal intubation is now almost routinely performed during general anesthesia. Clearly, any patient who has recently eaten or has intestinal obstruction should be managed by rapid intubation. Tracheal intubation is also usually mandatory for patients requiring positive-pressure ventilation (eg, during thoracotomy or when neuromuscular blocking drugs are given). When the patient must be placed in a position other than supine, endotracheal intubation is often required.
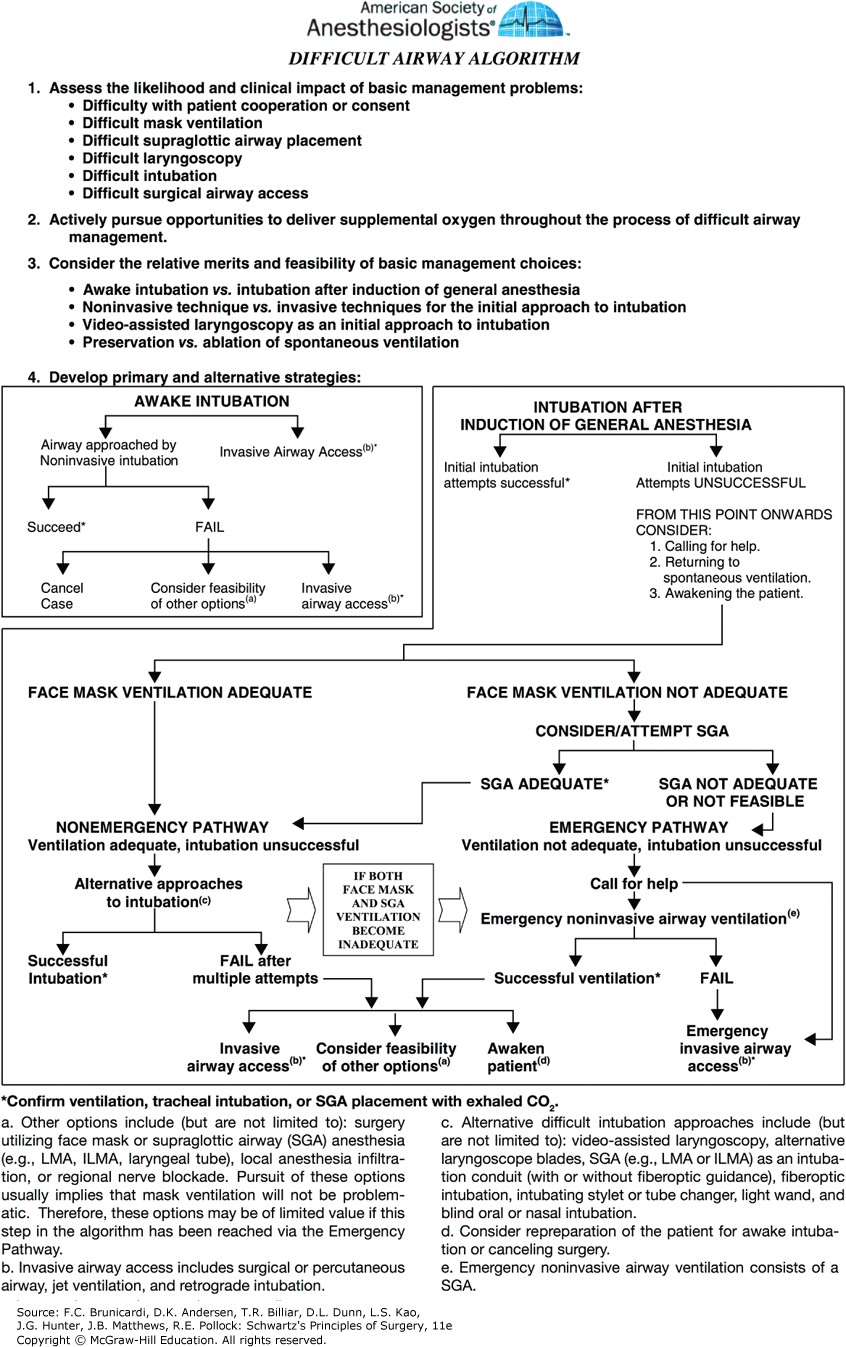
Figure legend: ASA difficult airway algorithm. (Reproduced with permission from Apfelbaum JL, Hagberg CA, Caplan RA, et al: Practice guidelines for management of the difficult airway: an updated report by the American Society of Anesthesiologists Task Force on Management of the Difficult Airway, Anesthesiology. 2013 Feb;118(2):251-270.)
Board Review Questions
1. A 40-year-old male status with juvenile onset diabetes mellitus, status post renal transplant 2 years prior, presents to an ambulatory surgery center for debridement of an AV fistula used in the past for dialysis. In spite of tight glycemic control, the patient has diabetic retinopathy and neuropathy. His renal function is normal and is no longer on dialysis. The patient has no risk factors for aspiration
This patient’s American Society of Anesthesiologists (ASA) physical status is:
A. class I
B. class II
C. class IIE
D. class III
E. class IV
2. Which of the following factors is not unique to the pediatric airway?
A. large occiput
B. long, narrow epiglottis
C. short neck
D. short trachea
E. posterior larynx
3. Which of the following statements regarding the LMA is true?
A. The patient must be kept breathing spontaneously.
B. It is contraindicated in asthmatic patients.
C. It is not safe in patients with hiatal hernias.
D. It is associated with a significant increase in bronchospasm compared to a conventional endotracheal tube.
E. It should not be used if a traditional mask airway provides adequate ventilation.
Answers
1. The correct answer is D. class III
2. The correct answer is E. posterior larynx
3. The correct answer is C. It is not safe in patients with hiatal hernias.

Create a Free MyAccess Profile
AccessMedicine Network is the place to keep up on new releases for the Access products, get short form didactic content, read up on practice impacting highlights, and watch video featuring authors of your favorite books in medicine. Create a MyAccess profile and follow our contributors to stay informed via email updates.