
Excessive alcohol consumption appears to account for 70–80% of all cases of chronic pancreatitis worldwide. However, the mechanisms associated with alcohol-induced acute pancreatitis and the progression to chronic pancreatitis remain uncertain. This relationship is even more confounding considering the facts that less than 10% of alcoholics actually acquire chronic pancreatitis and that there does not appear to be any specific level of alcohol consumption below which pancreatitis does not occur. Epidemiologic studies confirm that there is a genetic basis for alcoholic pancreatitis. Therefore, genetic susceptibility, environmental exposures, and the interaction between these factors must all be critical to the development of alcohol-induced chronic pancreatitis.
Ethanol appears to have direct toxic effects on the pancreas. These include the reduction of pancreatic blood flow and microcirculation, generation of free oxygen radicals in the pancreas, direct effects on acinar cell viability, and, when combined with cigarette smoke, the creation of pancreatic ischemia.4 Additionally, alcohol can directly activate pancreatic stellate cells—the main source of extracellular matrix in the pancreas.5
Recurrent subclinical episodes of pancreatitis induced by alcohol may ultimately lead to clinically evident inflammation and fibrosis. Since a small percentage of patients who drink ultimately present with chronic pancreatitis, a genetic susceptibility has been sought. To date, however, no candidate genes have been identified.
Although chronic pancreatitis is not primarily a surgical disease, the surgeon is frequently asked to evaluate and treat patients with this problem. The most common indication for operation is pain, but there are several other indications for surgery in this group.
Operation for persistent pain requires an assessment of the significance of the pain. Generally, operation may be indicated in patients whose pain interferes with the quality of their lives. For example, the attacks of pain may require frequent hospitalizations that interfere with school or employment. The patient may be unable to function productively because of the depression that often accompanies the chronic pain state. Nutrition may be impaired because the pain that eating produces, limits oral intake. The patient is often addicted to narcotics, but this may not be a contraindication to operation. For example, patients who undergo a pancreatic resection may develop exocrine insufficiency or diabetes if enough pancreas is removed. Although this may be an acceptable price to pay for pain relief in some patients, others might be unable to manage the dietary and insulin requirements that would ensue (e.g., patients who are addicted to narcotics and/or alcohol). However, even in patients with narcotic and/or alcohol addiction and a dilated duct, a duct decompression operation may be appropriate, because it almost never produces exocrine or endocrine insufficiency. Preoperative psychiatric evaluation may help the surgeon to decide about whether or not operation should be considered.
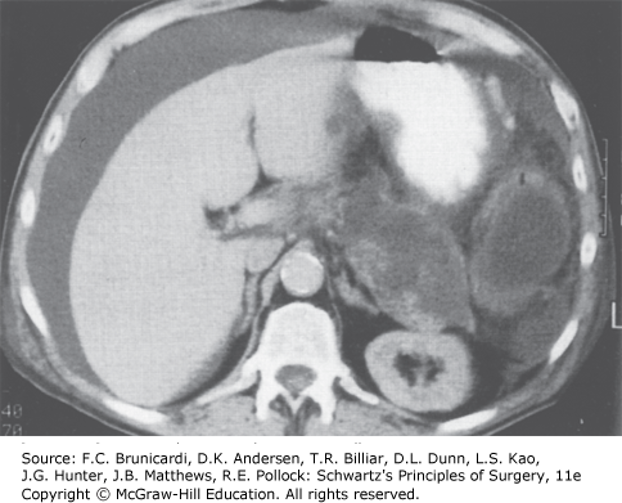
Pancreatic ascites. Computed tomographic scan of a patient with a ruptured pancreatic pseudocyst resulting in intraperitoneal pancreatic fluid. (Reproduced with permission from Cameron JL, Cameron AM: Current Surgical Therapy, 11th ed. Philadelphia, PA: Elsevier; 2014.)
Board Review Questions
1. A 54-year-old male, well known to you from multiple admissions for exacerbations of chronic alcoholic pancreatitis, comes to clinic requesting your opinion regarding surgical treatment for his pancreatitis. Which of the following sequelae of chronic pancreatitis would prevent him from being a candidate for longitudinal pancreaticojejunostomy (modified Puestow procedure)?
A. Disabling pain requiring the use of high doses of narcotics
B. Obstruction of the intrapancreatic common bile duct
C. Dilated pancreatic duct (6 mm) with no strictures
D. Diabetes
E. Multiple strictures along the entire length of a 9 mm duct
2. Which of the following is the initial medication used to treat pain in patients with chronic pancreatitis?
A. Enteric-coated pancreatic enzyme preparations
B. Non-enteric-coated pancreatic enzyme preparations
C. Octreotide
D. Somatostatin
3. The most common cause of chronic pancreatitis is
A. Alcohol consumption
B. Hypertriglyceridemia
C. Autoimmune pancreatitis
D. Hereditary pancreatitis
Answers
1. The correct answer is B. Obstruction of the intrapancreatic common bile duct
2. The correct answer is B. Non-enteric-coated pancreatic enzyme preparations
3. The correct answer is A. Alcohol consumption

Create a Free MyAccess Profile
AccessMedicine Network is the place to keep up on new releases for the Access products, get short form didactic content, read up on practice impacting highlights, and watch video featuring authors of your favorite books in medicine. Create a MyAccess profile and follow our contributors to stay informed via email updates.