
Malignant Tumors of the Thyroid
Essentials of Diagnosis
• History of irradiation to the neck in some patients.
• Painless or enlarging nodule, dysphagia, or hoarseness.
• Firm or hard, fixed thyroid nodule; ipsilateral cervical lymphadenopathy.
• Normal thyroid function; nodule stippled with calcium (x-ray), cold (radioiodine scan), solid (ultrasound); positive or suspicious cytology.
• Family history of thyroid cancer.
General Considerations
An appreciation of the classification of malignant tumors of the thyroid is important, because thyroid tumors demonstrate a wide range of growth and malignant behavior. At one end of the spectrum is papillary adenocarcinoma, which often occurs in young adults, grows very slowly, metastasizes through lymphatics, and is compatible with long life even in the presence of metastases. At the other extreme is undifferentiated carcinoma, which appears later in life and is non-encapsulated and invasive, forming large infiltrating tumors composed of small or large anaplastic cells.
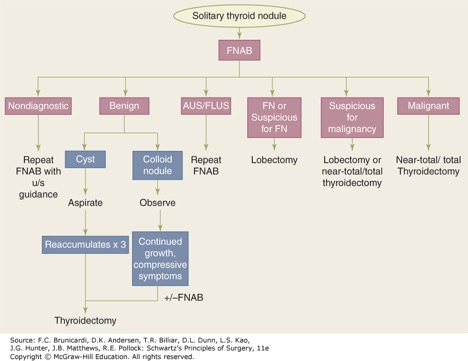
Most patients with anaplastic thyroid carcinoma succumb as a consequence of local recurrence, pulmonary metastasis, or both within 6 months. Between these two extremes are follicular, Hürthle cell, and medullary carcinomas, sarcomas, lymphomas, and metastatic tumors. The prognosis depends on the histologic pattern, the age and sex of the patient, the extent of tumor spread at the time of diagnosis, whether the tumor takes up radioiodine, and other factors. Evaluation of solid thyroid nodules to determine the nature and management is mainly informed by fine needle aspiration biopsy for cytology assessment (Figure).
Board Review Questions
1. Choose the one best response to this question.
A 35-year-old female presents with a painless midline mass above the hyoid bone for the past 4 months. She denies any history of neck radiation or previous surgery. The mass is 2 x 2 cm on physical examination and elevates on deglutination. What is the most common malignancy associated with this condition?
A. follicular
B. Hürthle cell
C. anaplastic
D. medullary
E. papillary
2. Choose the one best response to this question.
Which of the following statements about iodine-131 is false?
A. It is trapped and organified by the thyroid gland.
B. It may destroy residual occult microscopic foci of papillary and follicular malignancies.
C. There is no increase incidence of malignancy associated with radiation exposure.
D. It can safely be used in pregnancy.
E. It is not trapped in thyroid metastases and lymphoma.
3. Choose the one best response to this question.
A 20-year-old marfanoid male with bilateral thyroid tender lesions has evidence of submucosal neuromas, diarrhea, and facial flushing. A FNA of the nodules is performed, which demonstrates medullary thyroid carcinoma. Which is the recommended treatment after the possibility of pheochromocytoma is definitely excluded?
A. total thyroidectomy with postoperative calcitonin monitoring
B. total thyroidectomy with postoperative iodine-131 treatment
C. ipsilateral thyroid lobectomy with ultrasound examination of the contralateral lobe
D. total thyroidectomy with postoperative chemoradiation therapy
E. excisional biopsy with permanent pathology examination
Answers
1. The correct answer is E. papillary
2. The correct answer is C. There is no increase incidence of malignancy associated with radiation exposure
3. The correct answer is A. total thyroidectomy with postoperative calcitonin monitoring

Create a Free MyAccess Profile
AccessMedicine Network is the place to keep up on new releases for the Access products, get short form didactic content, read up on practice impacting highlights, and watch video featuring authors of your favorite books in medicine. Create a MyAccess profile and follow our contributors to stay informed via email updates.