NAPLEX® Review Question of the Week: Venturing Vancomycin

DR is a 41-year-old male. DR is in the hospital for native valve (aortic) MRSA endocarditis. You are the pharmacist on the floor responsible for vancomycin dose adjustments. He is on day 3 of treatment and his past medical history and labs are below:
PMH: HTN, PWID, HLD
Home Medication List:
DR is not currently taking any medications from home because he has not seen a provider in 3 years.
In-patient medication list:
Vancomycin 1500 mg IV Q12h
Heartburn Relief Max St 20 mg PO q24h
Elonox 40 mg SC q24h
Tylenol 325 mg PO q6h PRN for pain
Lisinopril 10 mg PO QD
Vitals:
Ht: 6’1 ft
Wt: 83 kg
BP: 134/81mmHg
SpO2: 97%
Pain level: 2
Temperature: 99.9 F
Heart rate: 88 BPM
|
|
Day 1 |
Day 2 |
Day 3 |
|
Scr (mg/dL) |
1 |
1.1 |
1.1 |
|
Vancomycin trough level (mg/L) |
— |
17 |
22 |
How should you adjust DR’s vancomycin dosing? The trough level on day 3 was before his sixth total dose (received no loading dose).
A. Vancomycin 1750 mg IV Q24h
B. Vancomycin 750 mg IV Q12h
C. Vancomycin 1250 mg IV Q12h
D. Vancomycin 1500 mg IV Q24h
Answer with Rationale
Vancomycin protocols including therapeutic drug monitoring (TDM) are one of the most common practices for pharmacists in hospital systems. Knowing how to adjust vancomycin levels based on goal trough, AUC, and CrCl is essential for keeping patients at goal. The goal trough for invasive MRSA infections is 15-20 mcg/mL while troughs of 10-15 mcg/mL are often used for other infections or noninvasive MRSA infections. AUC-based monitoring with a goal of 400-600 is often recommended due to potential decreased risk of nephrotoxicity compared to trough-based monitoring. This requires a calculator or software compared to a trough-based approach which only requires the lab draw. While some hospitals have adopted AUC-based monitoring due to its potential benefit in decreasing nephrotoxicity, many hospitals still use a trough-based approach.
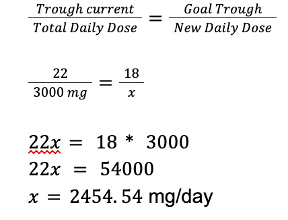
For this case, a simple way to adjust vancomycin is when a patient is at steady state and has stable renal function, you can do a ratio and proportion calculation similar to the below to get a good estimate for an adjustment. The goal trough for invasive MRSA infection is 15-20 mcg/mL so we the middle of this range is 17.5 or 18 if we round.
A. Incorrect. This would increase DR's total daily dose and increase his risk for nephrotoxicity.
B. Incorrect. This would give DR a suboptimal dose of vancomycin (trough below 15) and potentially impair its effectiveness considering the severity of his infection (MRSA endocarditis).
C. Correct. This would give DR a correct new dose to equal 2500 mg for a total daily dose.
D. Incorrect. This adjustment would provide too low of a trough and could increase his risk for clinical failure.
Brand/Generics covered: Vancomycin (Vancocin), Famotidine (Heartburn Relief Max St), Enoxaparin (Elonox), Acetaminophen (Tylenol), Carvedilol (Coreg), Spironolactone (Aldactone), Lisinopril (Prinivil)
Naplex Core Competencies Covered:
2.2 Brand, generic
4.1 Patient parameters or laboratory measures
4.2 Quantities of drugs to be dispensed or administered
4.4 Dose conversions
4.5 Drug concentrations, ratio strengths
4.9 Pharmacokinetic parameters
Dr. Christopher M. Bland is the Albert W. Jowdy Professor in Pharmacy Care at the University of Georgia College of Pharmacy at the Southeast GA campus in Savannah, GA. Dr. Bland has nearly 25 years of academic and clinical experience both in the inpatient and community patient care settings. He is a Fellow of both the Infectious Diseases Society of America as well as the American College of Clinical Pharmacy and has been named Teacher of the Year at the University of Georgia College of Pharmacy. He is co-author of the book "InteGREAT: A Guidebook for Creating Great Healthcare Teams."
He is co-founder of the Southeastern Research Group Endeavor, SERGE-45, with nearly 100 practitioners across 14 states involved. Dr. Bland serves as Associate Editor for the NAPLEX Review Guide 4th edition as well as upcoming 5th edition, as well as the Editor-In-Chief for the Question of the Week. He has provided hundreds of hours in live, interactive NAPLEX reviews for more than 10 Colleges/Schools of Pharmacy over the course of his career.

Create a Free MyAccess Profile
AccessMedicine Network is the place to keep up on new releases for the Access products, get short form didactic content, read up on practice impacting highlights, and watch video featuring authors of your favorite books in medicine. Create a MyAccess profile and follow our contributors to stay informed via email updates.