NAPLEX® Review Question of the Week: Dilantin Dilemma

CX, a 43-year-old male, presented to the ED after being found unconscious in his office at home by his wife.
PMH: Diabetes, Hyperlipidemia, Epilepsy (Generalized Tonic-Clonic)
Weight 80 kg, Height 71 in
Vitals: BP 145/82 mmHg, HR 97 bpm
Labs upon arrival:
A1c 5.9%
TC 147 mg/dL, LDL 65 mg/dL, HDL 38 mg/dL, TG 102 mg/dL
SCr 0.7 mg/dL, Albumin 3.0 g/dL
Current medications:
Metformin 1000 mg BID
Atorvastatin 20 mg QD
Levetiracetam 1000 mg BID
Upon arrival to the hospital, CX began having continuous tonic-clonic seizures for about 8 minutes, which was consistent with status epilepticus (SE). He was quickly intubated, and a dose of Ativan 4 mg IV was administered as initial emergent treatment. Despite receiving a 2nd dose of Ativan, CX continued to seize over the next few minutes. The ED physician determined that urgent therapy is needed and decided to give the patient Dilantin 1600 mg (20 mg/kg) as a loading dose infused over 30 minutes. CX remains in SE even after the infusion was finished, which prompted the physician to obtain a phenytoin level to determine the next steps.
Total phenytoin level 5.6 mcg/mL
What is CX’s corrected phenytoin level, and is it subtherapeutic or supratherapeutic?
A. 6 mcg/mL; subtherapeutic
B. 6 mcg/mL; supratherapeutic
C. 8 mcg/mL; subtherapeutic
D. 8 mcg/mL; supratherapeutic
Answer with Rationale
Status epilepticus (SE) is a medical emergency characterized by at least 5 minutes of continuous clinical and/or electrographic seizure activity or recurrent seizure activity without recovery between seizures. Delays in care can lead to significant morbidity or mortality. Acute processes (cerebrovascular event, cardiac arrest, metabolic disturbances, drug toxicity/withdrawal, CNS infection, head trauma, etc.) and chronic processes (anticonvulsant withdrawal, chronic alcohol use, CNS tumors, etc.) can both cause an individual to go into SE. Complications of SE include increased systemic BP, hyper- or hypoglycemia, hyperkalemia that can lead to arrhythmias, lactic acidosis, neurologic damage, etc. Status epilepticus requires prompt and organized treatment, with simultaneous supportive care (airway, breathing, circulation) and administration of antiepileptic drug (AED) therapy.
For patients with CrCl > 10 mL/min, the process for calculating corrected phenytoin in our patient is as follows:
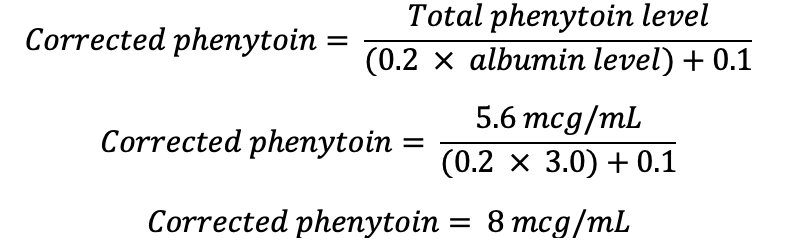
The therapeutic range of phenytoin to target in patients treated for SE is 10-20 mcg/mL for total phenytoin levels and 1-2 mcg/mL for free phenytoin levels.
Answers A & B are incorrect. Albumin is a protein that serves as a major source of drug binding. Since phenytoin is highly protein-bound (90%), correction for hypoalbuminemia is needed when albumin is ≤ 3.2 g/dL. Since CX’s albumin was 3.0 g/dL, a corrected phenytoin level must be calculated for CX to accurately access his treatment.
Answer C is correct. CX’s true total phenytoin level, after correction for hypoalbuminemia, is 8 mcg/mL, as calculated above. This value is below the therapeutic range of 10-20 mcg/mL.
Answer D is incorrect. CX’s true total phenytoin level, after correction for hypoalbuminemia, is 8 mcg/mL, as calculated above. This value is NOT above the therapeutic range of 10-20 mcg/mL.
Generic/Brand: Metformin (Glucophage), Atorvastatin (Lipitor), Levetiracetam (Keppra), Lorazepam (Ativan), Phenytoin (Dilantin)
NAPLEX Core Competencies Covered:
- 1.5 – Signs or symptoms of medical conditions, healthy physiology, etiology of diseases, or pathophysiology
- 2.2 – Commercial availability; prescription or non-prescription status; brand, generic, or biosimilar names; physical descriptions; or how supplied
- 4.1 – Patient parameters or laboratory measures
- 4.5 – Drug concentrations, ratio strengths, osmolarity, osmolality, or extent of ionization
Dr. Christopher M. Bland is the Albert W. Jowdy Professor in Pharmacy Care at the University of Georgia College of Pharmacy at the Southeast GA campus in Savannah, GA. Dr. Bland has nearly 25 years of academic and clinical experience both in the inpatient and community patient care settings. He is a Fellow of both the Infectious Diseases Society of America as well as the American College of Clinical Pharmacy and has been named Teacher of the Year at the University of Georgia College of Pharmacy. He is co-author of the book "InteGREAT: A Guidebook for Creating Great Healthcare Teams."
He is co-founder of the Southeastern Research Group Endeavor, SERGE-45, with nearly 100 practitioners across 14 states involved. Dr. Bland serves as Associate Editor for the NAPLEX Review Guide 4th edition as well as upcoming 5th edition, as well as the Editor-In-Chief for the Question of the Week. He has provided hundreds of hours in live, interactive NAPLEX reviews for more than 10 Colleges/Schools of Pharmacy over the course of his career.

Create a Free MyAccess Profile
AccessMedicine Network is the place to keep up on new releases for the Access products, get short form didactic content, read up on practice impacting highlights, and watch video featuring authors of your favorite books in medicine. Create a MyAccess profile and follow our contributors to stay informed via email updates.