
The modern era for drug treatment of obesity began in the early 1990s after studies were published by Weintraub and colleagues that showed that fenfluramine and phentermine given in combination with behavioral modification could sustain weight loss in some patients for an extended period of time. Although this drug combination was eventually withdrawn from the market because of its association with the development of pulmonary hypertension and valvular heart disease, Weintraub's approach heralded a change in the medical community, where obesity increasingly came to be recognized as a chronic disease process that warranted sustained medical attention and treatment.
Medical treatments for obesity have evolved over the past several decades as new drugs have been developed and introduced to the market. Medications that are approved for use for weight loss in the United States can be broadly categorized as those that decrease food intake by suppressing appetite or increasing satiety, and those that decrease nutrient absorption. Appetite suppressants are believed to work by increasing the availability of neurotransmitters such as norepinephrine, serotonin, and dopamine, which suppress appetite. Sibutramine works by inhibiting the uptake of these neurotransmitters. This drug may also stimulate thermogenesis, although this effect is modest and constitutes only 3–5% of the average person's resting metabolic rate. Randomized controlled trials indicate that the average patient will lose approximately 3–4 kg over 8–52 weeks of treatment. All subjects regained weight after treatment was discontinued.
Orlistat (Xenical) and sibutramine are the only FDA-approved medications to treat obesity. Orlistat reduces nutrient absorption by binding to gastrointestinal lipase and prevents the hydrolysis of dietary fat into absorbable free fatty acids and monoacylglycerols. Patients who are treated with orlistat excrete about a third of the dietary fat that they consume in their stools and can be expected to lose about 9% of their baseline weight on average. Randomized controlled trials also indicate that patients treated with orlistat tend to regain all of the weight that was lost when treatment is ended.
Thus, pharmacotherapy typically induces relatively small amounts of weight loss, in the range of 3–5 kg over 6 months. Similar outcomes are to be expected from behavioral counseling. Although long-term medical therapy can decrease the likelihood of a given patient regaining the lost weight, long-term data on the safety and efficacy of using any medication is sparse. As of 2002, there were no long-term randomized controlled trials demonstrating that prescription weight loss medications were safe or efficacious in children less than 16 years of age.
Despite the lack of durable success with medical therapy in many obese patients, the relationship between weight loss and reduction of much, if not all, of the risk of excess morbidity and mortality is well established. Loss of as little as 5–10% of pretreatment weight improves blood glucose control in type II diabetes, hypertension, and cardiovascular disease. Loss of 10 kg of body weight is associated with a 20–25% decrease in mortality from all causes, including 30–50% reductions in deaths related to diabetes and cancer.
Bariatric surgery should be offered to appropriate patients with BMIs of 40 kg/m2 or greater (or between 35 and 40 kg/m2 if significant medical comorbidities are present) who have failed medical treatment, nutritional treatment, lifestyle changes, behavioral modification, or other conservative therapies. Candidates for surgical therapy must be willing and able to comply with postoperative dietary recommendations, exercise, and follow-up requirements. Patients who have ongoing drug or alcohol dependency, who are unstable or otherwise unfit psychiatrically, or who are unable to undergo general anesthesia should not undergo bariatric surgery.
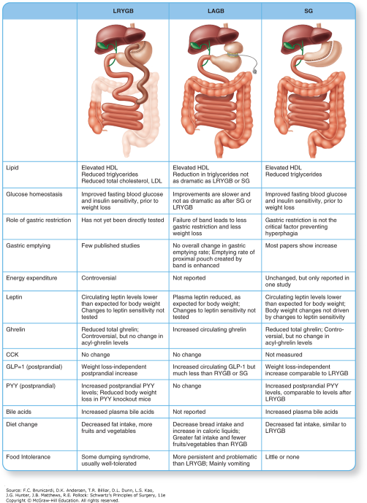
Mechanisms of effect: comparison of Roux-en-Y Gastric Bypass, Gastric Band Placement, and Sleeve Gastrectomy.
Quick Test Board Review Questions
1. Which of the following is associated with or caused by obesity?
A. Cluster headaches
B. Pseudotumor cerebri
C. Liposarcoma
D. Fat embolism
2. A bilipancreatic diversion (BPD) with duodenal switch is best characterized as a
A. Restrictive procedure
B. Malabsorptive procedure
C. Combination restrictive and malabsorptive procedure
D. None of the above
3. What percent of morbidly obese patients are able to successfully lose weight and maintain that weight loss by eating fewer calories and increasing the amount of exercise they do?
A. <5%
B. 5% -10%
C. 10% - 15%
D. >15%
Answers
1. The correct answer is B. Pseudotumor cerebri
2. The correct answer is C. Combination restrictive and malabsorptive procedure
3. The correct answer is A. <5%

Create a Free MyAccess Profile
AccessMedicine Network is the place to keep up on new releases for the Access products, get short form didactic content, read up on practice impacting highlights, and watch video featuring authors of your favorite books in medicine. Create a MyAccess profile and follow our contributors to stay informed via email updates.