
Lung Cancer
Treatment for small cell carcinoma consists primarily of chemotherapy and radiation, though recent data indicate that for early disease (T1–T2 lesions and limited hilar adenopathy) resection may improve local control and result in increased long-term survival (as high as 50%), particularly when combined with postoperative chemotherapy. Treatment for non-small cell lung cancer, however, varies with stage.
Early-stage disease (stage I/II) has historically been treated with surgery alone. However, the results of several randomized prospective trials involving adjuvant chemotherapy for early (Ib and higher) non-small cell lung cancer suggest benefit. Locally advanced but surgically resectable disease (stage IIIA) is currently best treated with combined-modality therapy utilizing induction chemotherapy or chemoradiotherapy followed by surgery and, if necessary, postoperative radiotherapy. Locally advanced and surgically unresectable disease (stage IIIB) is best managed with concurrent platinum-based chemotherapy and fractionated radiation therapy.
Metastatic disease (stage IV) is only poorly treated with chemotherapy. Radiotherapy in this case is reserved for symptomatic lesions. Combined-agent chemotherapy offers 2–3 months (20%) survival extension to advanced-stage patients. It has been shown to be cost-effective and improve quality of life and is generally well-tolerated by patients with reasonable performance status. New biologic agents are showing activity in clinical trials and should improve overall survival statistics. With advances in targeted and conventional therapies, the current overall survival (< 15% at 5 years) of patients with lung cancer can be improved.

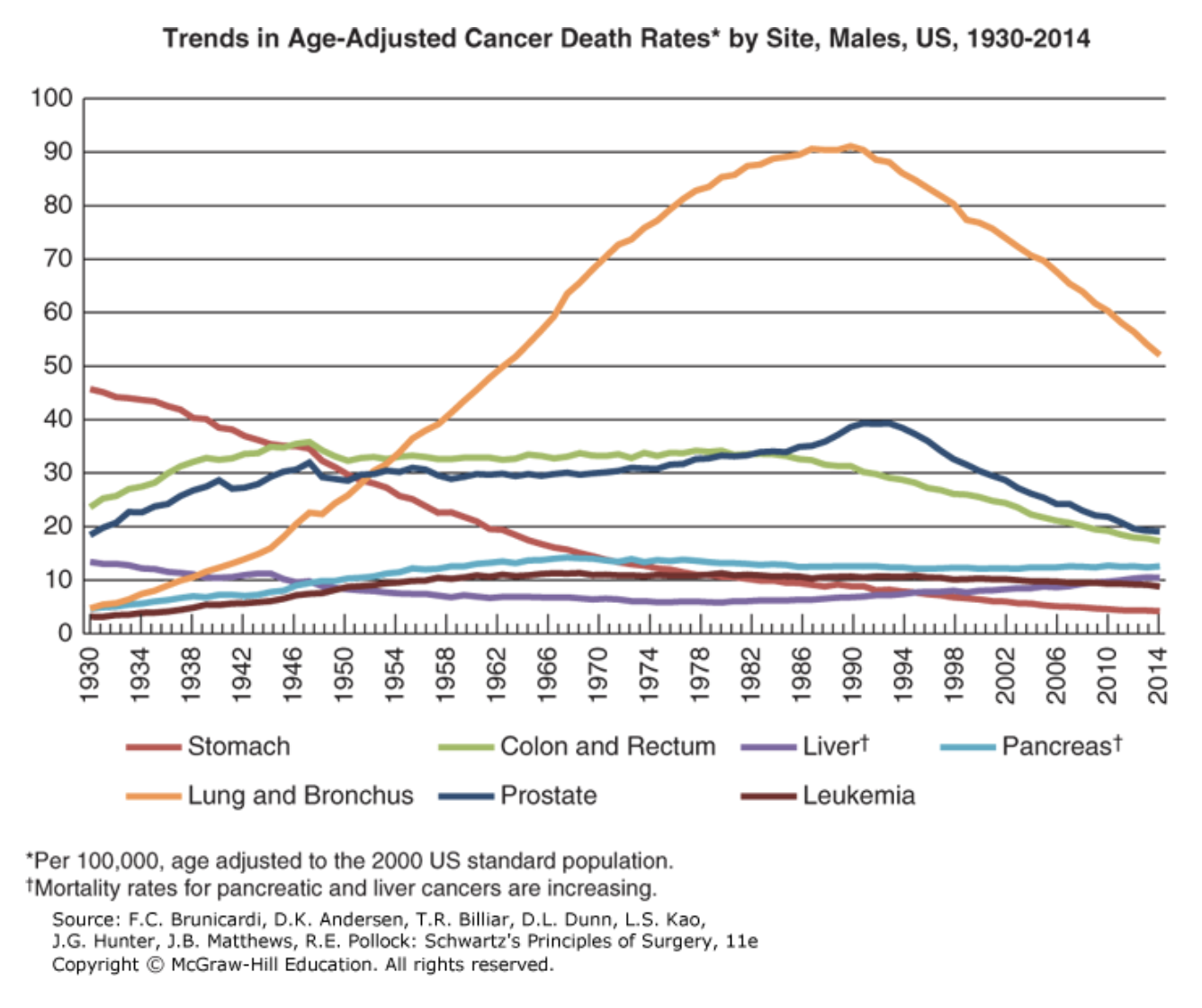
FIGURE LEGEND: Trends in death rates by sex for select cancers, United States, 1930 to 2014. A. Males. B. Female rates are age-adjusted to the 2000 U.S. standard population. Due to improvements in International Classification of Diseases (ICD) coding over time, numerator data for cancers of the lung and bronchus, colon and rectum, liver, and uterus differ from the contemporary time period. For example, rates for lung and bronchus include pleura, trachea, mediastinum, and other respiratory organs. (Adapted with permission from Siegel RL, Miller KD, Jemal A: Cancer Statistics, 2017, CA Cancer J Clin. 2017 Jan;67(1):7-30.)
Board Review Questions
1. A patient with lung cancer who presents with chest wall pain is most likely to have:
A. Squamous cell carcinoma
B. Small cell carcinoma
C. Adenocarcinoma
D. Bronchoalveolar carcinoma
2. The treatment of choice for a patient with a Pancoast tumor, no metastases, and good pulmonary function is:
A. Surgical resection followed by radiation therapy
B. Surgical resection followed by chemotherapy and radiotherapy
C. Induction chemotherapy followed by surgical resection
D. Induction chemotherapy and radiotherapy followed by surgical resection
3. The lymphatic drainage from the pulmonary (N1) nodes of the lung terminates in the lymphatic sump of Borrie which, on the right side, is located:
A. Around the bronchus intermedius
B. In the intralobar fissure
C. In the posterior mediastinum
D. At the level of the carina
Answers
1. The correct answer is C. Adenocarcinoma
2. The correct answer is D. Induction chemotherapy and radiotherapy followed by surgical resection
3. The corrrect answer is A. Around the bronchus intermedius

Create a Free MyAccess Profile
AccessMedicine Network is the place to keep up on new releases for the Access products, get short form didactic content, read up on practice impacting highlights, and watch video featuring authors of your favorite books in medicine. Create a MyAccess profile and follow our contributors to stay informed via email updates.