Week 8 Q&A
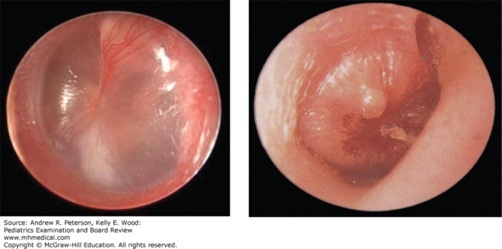
She has been healthy and this is her first illness. She has no known drug allergies. Her mother reports that several members of the family “had a cold” last week and the patient had several days of coughing and rhinorrhea that seemed to improve. Physical exam reveals an ill-appearing infant with a temperature of 39.2°C (102.5°F) and a right tympanic membrane (TM) that is erythematous and bulging with white fluid present behind the TM. You perform pneumatic otoscopy and do not appreciate any movement of the TM. (See image below). You explain to the mother that the child has a right-sided acute otitis media (AOM).
Which of the following is the most appropriate initial treatment for this patient?
A. Clindamycin
B. Cefuroxime
C. Cefdinir
D. Amoxicillin and clavulanic acid (Augmentin)
E. Amoxicillin
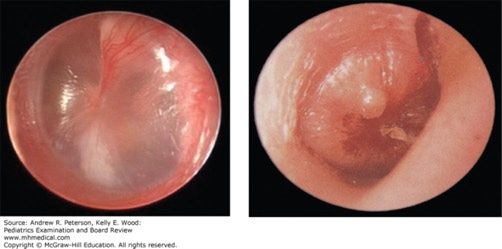
Acute otitis media. (A) A normal tympanic membrane is shown with a shiny light reflex. (B) The tympanic membrane is inflamed (red), bulging, and has a purulent effusion consistent with acute otitis media. The light reflex is gone. (Used with permission from Dr. Shelagh Cofer, Department of Otolaryngology, Mayo Clinic.)
Explanation:
The correct answer is “E.” According to the 2013 American Academy of Pediatrics (AAP) Clinical Practice Guideline for the diagnosis and management of AOM in children, first-line therapy for AOM is high-dose amoxicillin (80–90 mg/kg of body weight/day divided twice daily). S. pneumoniae often is resistant to lower dose amoxicillin. This resistance mechanism is via alteration of penicillin-binding proteins (not beta-lactamase production) and can usually be overcome by increasing the dose of amoxicillin. If the patient (1) has been treated with amoxicillin in the past 30 days, (2) has a history of recurrent AOM unresponsive to amoxicillin (3) has concurrent purulent conjunctivitis, or (4) has shown no improvement after 48 hours of amoxicillin therapy, then clinicians should prescribe an antibiotic with additional beta-lactamase coverage (option “D”). Concurrent conjunctivitis suggests H. influenzaeinfection. H. influenzae often is resistant to penicillin via beta-lactamase production. Addition of the beta-lactamase inhibitor clavulanate usually is able to overcome this resistance mechanism. If the patient has a penicillin allergy, then alternative agents include cefdinir, cefuroxime, or cefpodoxime. If the patient is unable to take oral medications or compliance is a concern, then you may consider ceftriaxone 50 mg/kg given intramuscularly once daily for 3 days. Remember that AOM is painful and all patients should receive oral pain medication as well. Children younger than 2 years of age should be treated for 10 days, children older than 2 years should be treated for 7 days, and children older than 6 years should be treated for 5 days.
Go to Access Pediatrics for the recommendations on the initial management of AOM.
Source: Peterson AR and Wood KE. Pediatrics Examination and Board Review. New York, NY: McGraw-Hill Education; 2017.




Create a Free MyAccess Profile
AccessMedicine Network is the place to keep up on new releases for the Access products, get short form didactic content, read up on practice impacting highlights, and watch video featuring authors of your favorite books in medicine. Create a MyAccess profile and follow our contributors to stay informed via email updates.