Dermatology Question of the Week: Medical Mysteries

Question:
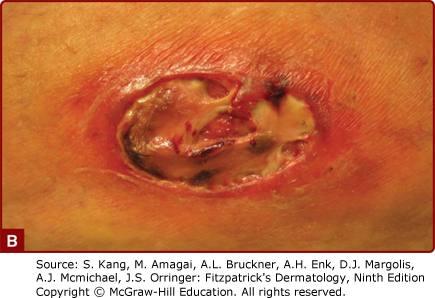
A 56-year-old patient with a past medical history of Crohn's disease and uncontrolled diabetes mellitus presents to you with a 1-week history of a very tender enlarging ulceration on the lower leg pictured below.
You perform a biopsy and tissue culture which shows significant neutrophilic infiltrate and no microorganism growth confirming your suspicion of pyoderma gangrenosum. You decide to initiate cyclosporine for rapid symptom relief. Which of the following is not a potential side effect of this medication?
Answers:
A. Hypertension
B. Hypokalemia
C. Hypomagnesemia
D. Hypertriglyceridemia
E. Increased uric acid
F. Increased risk of infections
G. Renal toxicity
Rationale:
Pyoderma gangrenosum (PG) is a neutrophilic dermatosis that, in the ulcerative form, presents as a tender ulcer with an undermined border, surrounded by a violaceous rim, and heals with cribiform scarring. PGs are sometimes associated with a systemic disease, including but not limited to ulcerative colitis, Crohn's disease, arthritis, and leukemia. Prednisone is typically used to decrease the inflammatory infiltrate and provide symptomatic management. In the vignette above, the treating physician opted for an alternative treatment to prednisone given the underlying uncontrolled diabetes. Cyclosporine is a first-line therapy for PGs and frequent laboratory monitoring is required due to the risk of hyperkalemia, hypomagnesemia, hypertriglyceridemia, and increased uric acid levels. Headache, nausea, vomiting, diarrhea, gingival hyperplasia, and hypertrichosis are other common side effects. Cyclosporine is typically dosed at 2.5-5mg/kg/d divided over two daily doses.
Correct answer: B Hypokalemia
Hyperkalemia can be seen in patients treated with cyclosporine and should be monitored closely to mitigate the risk of arrhythmia.
Incorrect answers:
A. Hypertension can be seen with the use of cyclosporine and should be monitored regularly. Extra caution should be taken in patients with underlying hypertension.
C. Hypomagnesemia can occur with cyclosporine and requires monitoring and correcting abnormal Mg levels to avoid the risk of seizures.
D. Hypertriglyceridemia can occur with cyclosporine use and should be monitored to avoid reaching significantly elevated levels.
E. Increased uric acid can occur with cyclosporine.
F. Cyclosporine is an immunosuppressive agent and patients are at increased risk of infections.
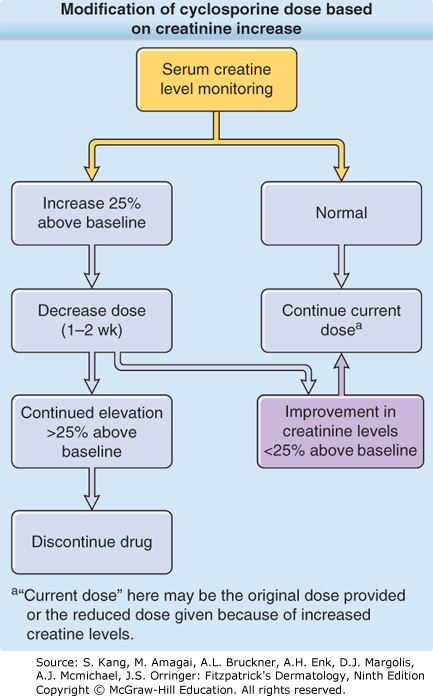
G. Cyclosporine can cause both acute and chronic renal failure. Patients' creatinine should be checked regularly and cyclosporine dosing should be adjusted accordingly as noted in the figure below. The use of cyclosporine should be limited to a maximum of 6-12 months to avoid the development of chronic renal failure secondary to this medication which in many patients is permanent.
Additional reading at Chapter 37: Pyoderma Gangrenosum and Chapter 192: Immunosuppressive and Immunomodulatory Drugs
I am a general dermatologist practicing at an academic medical center in Danville, PA. I see both adult and pediatric patients and also perform various surgical procedures. I have a special interest in Hidradenitis Suppurativa (HS) and am the founder of our HS specialty clinic where we treat patients medically and surgically (deroofing, excision, staged CO2 excision with marsupialization, Nd:YAG). I am actively involved in resident education and am passionate about medical education. Additional interests include autoimmune bullous disorders, dermatomyositis, and procedural dermatology.

Create a Free MyAccess Profile
AccessMedicine Network is the place to keep up on new releases for the Access products, get short form didactic content, read up on practice impacting highlights, and watch video featuring authors of your favorite books in medicine. Create a MyAccess profile and follow our contributors to stay informed via email updates.