Dermatology Question of the Week: Deductive Dermpath

Question:
A 20-year-old female presents for recurring findings seen in the photograph below. Multiple family members have similar rashes. You perform a biopsy which shows the findings seen on H&E and below. Which genetic mutation is seen in this condition?

Answers:
A. PSORS1
B. ATP2C1
C. ATP2A2
D. Uroporphyrinogen decarboxylase
E. Keratin 5
Rationale:
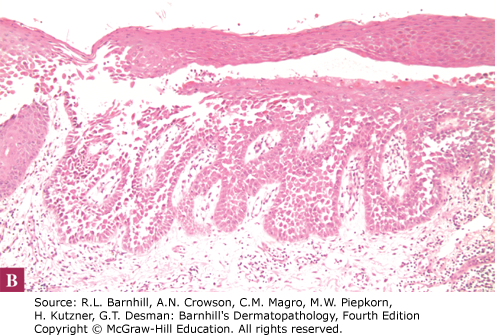
The key to identifying the correct answer requires the recognition of an intraepidermal vesicular process with significant acantholysis (separation of keratinocytes). The differential diagnosis from the clinical photograph includes intertrigo, inverse psoriasis, candidiasis, amicrobial pustulosis of the folds, granular parakeratosis, pemphigus vegetans, Hailey Hailey disease, etc.
Correct answer: B
ATP2C1 mutation is seen in Hailey Hailey disease. In the photograph above, the patient has a vegetative pink lightly scaly plaque on the right axilla and the H&E shows significant acantholysis reminiscent of a dilapidated brick wall. Hailey Hailey disease, also known as Familial benign pemphigus, commonly presents as recurrent vesicles on a pink/red base in the intertriginous areas and typically presents in adolescence/young adults. Two mnemonics for remembering the association between Hailey Hailey disease and ATP2C1, are "I want 2 C Hailey's comet 1 day" or "in order to Hail a cab, you need 2C1."
Incorrect answers:
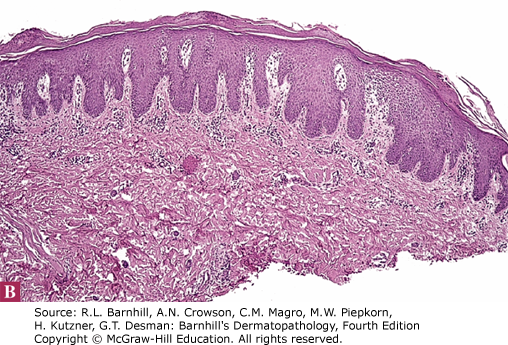
A. PSORS1 is a locus associated with psoriasis. Although the clinical image above may be confused for inverse psoriasis, the pathology clearly shows significant acantholysis. Psoriasis typically shows acanthosis (not acantholysis), parakeratosis, neutrophils in the stratum corneum, and tortuous blood vessels in the dermal papillae. An example is shown below.
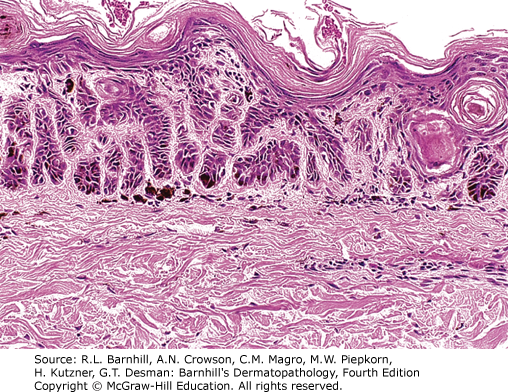
C. ATP2A2 mutation is seen in Darier disease. Darier disease typically presents with reddish brown crusted keratotic papules coalescing into plaques with a follicular predominance in seborrheic areas. On histology, Darier disease demonstrates significant dyskeratosis with grains and corp ronds and less acantholysis than Hailey Hailey disease. An example is shown below.

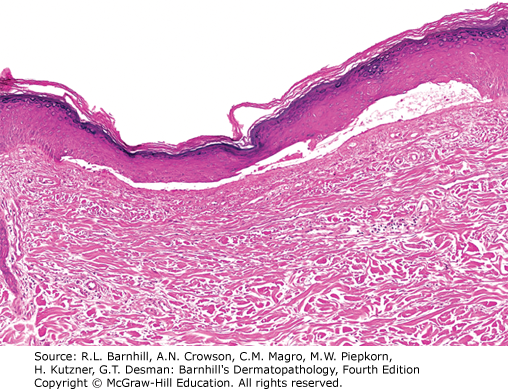
D. Mutations in uroporphyrinogen decarboxylase are seen with inherited porphyria cutanea tarda (PCT). PCT typically presents as vesicles, bullae, scarring, and milia in sun-exposed sites such as the hands and hypertrichosis of the face. On histology, PCT demonstrates subepidermal bullae with pauci-inflammatory infiltrate as well as festooning of the dermal papillae. An example is shown below.
E. Mutations in keratin 5 can be seen in Dowling-Degos disease which presents clinically with reticulate pigmentation of the axillae and groin typically in the 3rd or 4th decade of life. On histology, Dowling-Degos disease shows branching, hyperpigmented rete ridges, the presence of horn cysts, and follicular involvement. Galli-Galli disease is a variant of Dowling-Degos and demonstrates foci of acantholysis in addition to the findings above. An example of Dowling-Degos disease is shown below.
Additional reading Chapter 7: Intraepidermal Vesiculopustular Diseases
I am a general dermatologist practicing at an academic medical center in Danville, PA. I see both adult and pediatric patients and also perform various surgical procedures. I have a special interest in Hidradenitis Suppurativa (HS) and am the founder of our HS specialty clinic where we treat patients medically and surgically (deroofing, excision, staged CO2 excision with marsupialization, Nd:YAG). I am actively involved in resident education and am passionate about medical education. Additional interests include autoimmune bullous disorders, dermatomyositis, and procedural dermatology.

Create a Free MyAccess Profile
AccessMedicine Network is the place to keep up on new releases for the Access products, get short form didactic content, read up on practice impacting highlights, and watch video featuring authors of your favorite books in medicine. Create a MyAccess profile and follow our contributors to stay informed via email updates.